London Borough of Richmond upon Thames: local authority assessment
Downloads
Overall summary
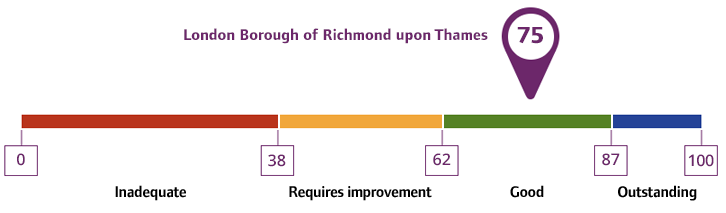
Local authority rating and score
Quality statement scores
Summary of people’s experiences
Care and support was planned and organised with people and people and unpaid carers described feeling listened to during assessments and were involved in decisions.
Feedback from unpaid carers showed that they valued being able to return for help when circumstances changed, which gave them reassurance and reduced stress.
Some people and unpaid carers said it could be confusing to access information across so many different systems and organisations. They also told us the local authority had taken steps to support people’s access to information about the local authority and partner organisations.
Some people, who self-funded their care and support, told us that finding the information they needed was a challenge. The local authority was committed to improving self-funders access information and staff across the local authority described sharing information on how to commission services and financial advice on how to pay for care.
People told us direct payments had improved outcomes and wellbeing. Unpaid carers told us direct payments supported them with their physical and mental health. However, feedback in relation to support with direct payments was mixed. One unpaid carer told us they had found the support helpful, however other unpaid carers said they did not have enough support with the system, and remained confused, in particular around the flexibility and restrictions when using a direct payment.
Some people told us transitions from children to adults’ services were not consistently planned or supported. Some unpaid carers highlighted gaps in support during transitions from children to adult services. An example of this was that unpaid carers told us clubs and breaks disappeared when young people turned 18, and although direct payments helped maintain some support there was a loss of structure and a risk of isolation.
People told us respite care was limited, although social workers acted when needed. A voluntary sector partner said there needed to be more choice in respite for unpaid carers.
People’s experiences reflected both positive and negative aspects of eligibility and decision-making in relation to adaptations. For example, some people described delays and unclear communication about eligibility for adaptations.
Summary of strengths, areas for development and next steps
Performance across key adult social care indicators demonstrated strong outcomes compared to national averages. All people lacking capacity were supported by an advocate, family member, or friend. A higher proportion of people received direct payments than the England average.
People’s feedback was also positive, in relation to accessing information and the provision of support helps them feel better about themselves.
According to the Adult Social Care Activity Report (ASCAR) 2024/25, 76.54% of long-term support clients received a review, significantly better than the England average of 59.13%. There were also significant levels of people receiving short-term support that no longer required further assistance. This included people aged 65+ remaining at home 91 days after discharge from hospital into reablement or rehabilitation services.
The local authority offered accessible care and support through various channels, including online, phone, email, and walk-ins. A well-structured front door process ensured effective triage and smooth transitions, minimising the need for people to repeat their stories. The local authority had commissioned advocacy services to support people and unpaid carers through assessment, review and safeguarding processes.
Assessments were person-centred and strengths-based, promoting independence and choice. Trauma-informed practices were embedded, with staff trained to support people respectfully and sensitively. Staff surveys showed high confidence and training levels, supporting the quality of care planning.
Care was coordinated across teams and partners agencies. Specialist teams managed complex referrals, and policies emphasised prevention and person-centred approaches, ensuring compliance with the Care Act and consistent, high-quality assessments.
There were no concerns about the timeliness of assessments for people and unpaid carers, and changes in need were addressed promptly. Efforts to manage and reduce waiting times were proactive and targeted.
People on waiting lists were contacted to monitor changes in their circumstances and connect them to community resources. Similarly, processes to ensure prioritisation of transition cases ensured people were assessed in advance of reaching the age of 18.
The local authority had adopted additional measures, including increasing staff capacity and encouraging front door teams to explore interim support options while full assessments were pending. These actions improved responsiveness and helped prevent crises.
Unpaid carers’ needs were treated as distinct from those they cared for, with separate assessments and support plans often included contingency planning. Carers appreciated measures like Carers Emergency Cards. Practical support such as direct payments and respite care enhanced carers’ wellbeing.
The local authority maintained a clear, transparent, and consistently applied framework for assessing and charging adults for care and support. Guidance documents were well-structured and accessible, with regularly reviewed procedures and policies that ensured transparency and accountability.
The local authority adopted a proactive, prevention-focused approach to care and support, working collaboratively with people, partners, and the community to promote independence and reduce reliance on formal services. This strategy was underpinned by access to reablement, community health initiatives, and digital tools.
Staff demonstrated creativity and commitment in using care technology and practical interventions to prevent escalation of needs, while initiatives like Making Every Contact Count (MECC) helped streamline support and reduce duplication. Housing and homelessness were key challenges, addressed through cross-sector collaboration and inclusive design, including a new homeless hub and specialist occupational therapy input. Prevention was embedded across the organisation, supported by a shared vision between Public Health and Adult Social Care.
Mental health support was enhanced through strategic partnerships, and the impact of the prevention strategy was monitored using outcome data.
The local authority prioritised access to equipment and home adaptations to support independence and reduce reliance on care packages. The Occupational Therapy team collaborated with frontline services and the Home Improvement Agency to ensure needs were met and to manage the Disabled Facilities Grant effectively. Trusted assessors in voluntary organisations provided minor aids, reducing duplication and unnecessary referrals.
Investment in smart care technology enabled personalised support and improved outcomes, benefiting both people and unpaid carers. The local authority also had an established responder service, however acknowledged that a small number of people were unable to access this service due to living alone and not having the minimum requirement for two named contacts. Staff told us that people who don’t have two local named contacts cannot access the responder service, and this lack of informal support could potentially lead to unnecessary hospital admission.
The local authority were exploring this issue and actively looking at ways to resolve the situation. Staff told us people can use smart digital alternatives, but this required people to have at least one family or friend as their named representative, but they may not need to live in the local area.
Following the collapse of the externally commissioned community equipment provider, the local authority responded swiftly by securing a new local supplier, prioritising those most at risk and maintaining communication with staff. While it was too early to assess the long-term impact, safe and effective interim arrangements were in place.
The local authority demonstrated a strong commitment to equality and inclusion by using detailed demographic and equality data to inform service design and reduce inequalities in care experiences and outcomes. It identified gaps in culturally responsive care and addressed underrepresentation of ethnic minorities in services through collaboration with community organisations and audits of support plans.
Barriers included digitally excluded groups, and initiatives like ‘Connect to Tech’ and dedicated refugee support teams helped to bridge access gaps. A Culturally Responsive Services Action Plan guided improvements in service specifications, workforce capability, and data monitoring. Equality Impact Assessments were used to mitigate risks and ensure inclusive service changes. The local authority embedded equality objectives into corporate plans.
There was a culture of continuous improvement and proactive learning from feedback from people which was systematically gathered and used to shape priorities and improve services. Co-production with people with lived experience and unpaid carers shaped services.
Staff training in cultural competence and gender identity supported inclusive care delivery. Continuous learning was promoted through staff forums and bite-size training, enhancing professional curiosity and confidence in addressing equality issues.
The local authority demonstrated strong and effective partnership working with health, social care, and community organisations, underpinned by clear governance, accountability, and information-sharing arrangements.
There were collaborative working arrangements in place, and innovative actions to support system wide improvements that would positively impact on people in Richmond. Strategic relationships with health partners and the voluntary sector enabled integrated care and innovation, while forums like the Urgent and Emergency Care Board facilitated collaborative responses to challenges such as hospital discharge.
Joint planning and commissioning improved service design and outcomes, and pooled budgets supported tailored services and innovation, including micro-grants for community-led initiatives.
We found evidence of strong governance and accountability, with clear structures at all levels ensure visibility, assurance, and compliance with Care Act duties. Robust risk management included embedded processes and proactive escalation routes were in operation.
Quality assurance processes and structured feedback mechanisms ensured continuous improvement and reinforced shared responsibility for care standards. These led to more coordinated care, quicker access to support, and reduced delays, with examples showing how joint working addressed urgent health needs and improved transitions.
Areas requiring further attention included communication arrangements between the emergency duty team and daytime teams, as there was a reliance on system notes rather than direct dialogue which limited opportunities to clarify urgent issues and could affect continuity of care.
We found transition arrangements and processes were well-established with structured tracking processes, regular multi-agency discussions and strong collaboration between adults’ and children’s services. However, evidence showed when young people turned 18, many of the clubs and short breaks they previously attended stopped. While some families received direct payments to arrange additional care, some unpaid carers felt this often placed responsibility on them to fill gaps resulting in additional pressure for families, reducing continuity of care and limiting opportunities for young people to maintain social networks.